
Author : Prof. Rasjid Skinner, Consultant Clinical Psychologist, Bradford
Key words : Islam, Psychology, Islamic Psychology
Background
The concept of Psychology, viewed in a clinical format, tends to present itself in the Western world as an objective universal science. The term ‘Western Psychology’ and its derivative therapies are however fundamentally rooted in western value systems, western paradigms of thought, and empirical studies mostly undertaken within ‘Western’ population samples (1,2).
Western Psychology and therapies are consequently ‘culture bound’ – its application cannot truly be claimed universal and has an uncertain relevance to those from non-western cultures, and to cultural sub-groups within the ‘West’, and even to ‘Western’ societies as the concept shifts culturally with time (3).
Beyond the western world, other cultures, usually from a much earlier starting point, have developed their own traditions of Psychology. These are described by Enriquez as ‘indigenous psychologies from within’ (2).
In Islamic civilisation, writings on Psychology, both in its theory and its clinical applications, begin early, – probably with Al-Kindi(801–873 CE), followed by Al-Balkhi, Al-Ghazali, and Ibn Arabi amongst others (4,5). All of these based their understanding of human psychology on Quranic sources and incorporated other sources as appropriate. The author was told that ʿIlm al-Nafs (academic psychology) was on the syllabus at Nishapur University by the 14th century C.E., and Ṭibb al-Nafs (Clinical Psychology/Psychiatry) by the 15th century C.E. Certainly by the late 14th century C.E. when the Ottoman mental hospital at Edirne was established, there was a developed understanding of mental disorders and of how they could be effectively treated.
There seems to have been a hiatus in the development of psychology from an Islamic tradition after the late medieval period. Arguably this was because what had already been developed, and practised by Hakims and others, was sufficient for a stable fiṭri based society, until Western Psychology began to significantly intrude into the Muslim world in the 1970s. This intrusion produced a reaction from Malik Badri, a British trained Clinical Psychologist, that resulted in the publication in 1979 of The Dilemma of Muslim Psychologists (1,6). In this work, Badri argued that Western Psychology contained elements antagonistic to Islamic precepts which, if not challenged, would result in (to use Enriquez’s term) a ‘colonisation of the mind’. Since then, there has been a growing international interest in developing an Islamically based psychology, and psychological therapies that are fitted to the increasing complex psychological problems of the modern age.
In the U.K., Abdullah Maynard and SabnumDharamsi began teaching a ‘mainstream’ accredited course in Islamic Counselling some 25 years ago. For the last 10 years, courses aimed at orientating existing clinicians to Islamic models have been taught at the Cambridge Muslim College and elsewhere in England. Some five years ago, Ihsaan and Inayat, consortia of Islamic psychological therapists, were established in West Yorkshire and Lancashire respectively. In 2017, Malik Badri established the International Association of Islamic Psychology to protect the integrity of the field, and to accredit therapists and training courses.
Defining Islamic Psychology
The International Association of Islamic Psychology defines Islamic Psychology as the Psychology that is based on an Islamic paradigm. Paradigm, from the Greek, being understood as an underlying foundational motif. Abdallah Rothman (7,8) has defined what constitutes an Islamic paradigm in psychology, and this definition has met with widespread acceptance.
Standing on this paradigm orientates the clinician in understanding pathology and its treatments, as well as indicating the conduct (adab) appropriate to the therapeutic relationship, and it establishes a standpoint from which to critique Western and other psychologies. The Psychology that derives from an Islamic paradigm is fundamentally distinct from culturally adapted or ‘Islamicized’ Western Psychology, and is a completely different field from ‘Islam and Mental Health’ (9).
An Islamic Model of the Self
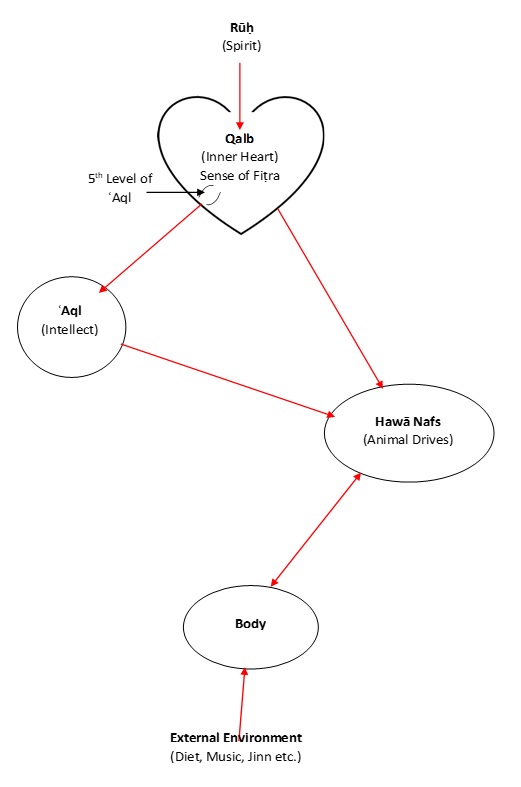
Fig. 1. An Islamic Model of the Self (8)
The model, exampled here, was first presented by the author as part of his paper to the IIIT London conference in 1989. It was devised after discussion with Islamic scholars available at the time in England, (in particular Shaykh Zahran Ibrahimand Muhtar Holland); and practicing clinicians including Alia Haeri and Hakim Salim Khan. The aim was to produce a simple diagrammatic model that would assist the clinician in makingdiagnoses and treatment decisions. It does not pretend to capture the full complexity and subtlety of Man’s nature. It is the model adopted by Ihsaan, the Bradford based Islamic Psychological therapy clinic, and is taught at the Cambridge Muslim College, and has been found acceptable to Islamic therapists over the last 30 years. It is not however the only model. Abdullah Rothmanhas published a diagrammatic model slightly different (10); and there are other authentic models. It is up to the therapist to decide which best assists their clinical practice.
Key Concepts
Quranic Arabic terms have a depth of meaning and nuance and have often been understood in different ways by classical scholars. The terms used in this here take an aspect of meaning which makes sense of psychological phenomenon, – broadly following the usage of Al-Ghazali (11).
Qalb
A distinguishing feature of Islamic Psychology is that it acknowledges a spiritual centre at the centre of the human being. Western Psychology, in the main, ignores or denies such a centre, – the main exception being the marginalised Psychology of Carl Jung. Some traditional scholars term the inner centre as ʿAql (see below), or Rūḥ (spirit), but Al-Ghazali mostly uses the term Qalb (heart).
The Qalb is perceived as containing an inherent sense of ‘fiṭra’ – what is natural and right, – and is open to divine inspiration (Rūḥ) – in the form of true dreams and inspired intuition for example. Generally speaking, the Eastern religions such as Buddhism do not conceptualise the inner self as open to divine inspiration: – or at least, not in the same way as do the Prophetic religions.
ʿAql
ʿAql can be translated as intellect, or the cognitive faculty. Al-Ghazali describesʿAql as having five functions. Four of these essentially describe the intellectual operations, such as logical reasoning, understood in Western cognitive psychology. The fifth function, however, is of a different level and can be considered as being part of and extending from the Qalb. This level of ʿAql is that which receives and articulates the knowledge of the heart (gnosis). It is this aspect of ʿAql which should direct the operations of the other parts, to avoid reasoning becoming disassociated from fiṭra and becoming (to paraphrase a Ḥadith) like ‘sorcery’.
The root meaning of the word ʿAql’ is shackle. Aql is normally understood as the faculty that shackles, or reins in, the forces in the Hawā. However, ʿAql (in its outer four functions) can also be seen to sometimes shackle the Qalb, – constricting the flow of gnosis coming from that source. When this happens, a transitory psychotic like state, or spiritual crisis, can occur as the ‘shackle’ is temporarily broken to allow new knowledge to be received. Jung describes experiencing such a state during the First World War period (12).
Hawā
‘The animal self’ refers to the instinctive drives and energies we require for our existence in this life. Colloquially, (even in Al-Ghazali’s day) these drivesare often referred to as ‘the nafs’. Particularly in the Islamic medical tradition, (Ṭibb), there is an understanding that the balance and type of these energies are closely related to diet.
The Body
In part, the body can be viewed as the base layer of the Self; – the carnal casing, necessary for this life but discarded at death. It is the vehicle for carrying out the instruction of the internal faculties (of the Qalb, ʿAql, and Hawā), and is the entree point for environmental forces (from food and drink, the atmosphere, mobile phones, jinn etc.) which then alchemise into internal energies, – particularly within the Hawā.
However, Islam is an embodied religion: for example, in the physical movements of the ritual prayer (ṣalāt); and the Prophet (peace be upon him) emphasised the spiritual significance of the ‘sunna sports’, – archery in particular. In one hadith, likening archery to a form of prayer (ḏikr). There is thus an understanding that the body has a subtle relationship with the Qalb and spiritual state.
Ibn ʿArabiis one scholar who deals with this aspect of the body (13). Taking the hadith relating how our body parts will bear witness, for or against us, on the Day of Judgement, Ibn ʿArabi conceives the body parts as having their own semi-autonomous existence, – their own ḏikr, and their own wish to worship God through the Human Being. This understanding underlies Islamic traditions of working with the body to remedy imbalances in mental or spiritual states and gives a perspective on ‘psycho-somatic’ symptomatology.
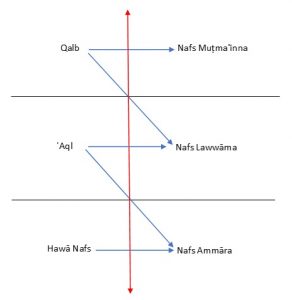
Fig. 2. Levels of States of Being (8)
Dynamics
Ḥadith relate that each child is born in‘fiṭra’, – that is, in a pure natural state absorbed in the awareness of God. Immediately after birth, however, the baby is pricked by Shayṭān.Thus, in this life, the Self is conceived as containing a continual struggle between the pull of fiṭra emanating from the Qalb, which seeks to bring the Self back to what is natural and right for the human being, and back into union with God; and the pull of Shayṭān in the opposite direction.
The three levels, or states, of the Self described in the Quran (Q. 12:53, 75:2, 89:27-28),Nafs Ammāra, Nafs Lawwāma, Nafs Muṭmaʾinna, can be seen as reflecting the outcome of this struggle at any point of time. Nafs Ammāra (the Compelling Self) thus refers to the state of the Self when it is dominated (compelled) by the lower energies of the Hawā. Nafs Muṭmaʾinna (the Well Pleasing, Contented Self), the state when the Self is under the direction of the Qalb. Nafs Lawwāma (the Remorseful Self) is the bridging state, in which the Self has awareness of its separation from fiṭra and closeness to the divine. The state of Nafs Lawwāma is critical for psychological work, as in that state, the individual can either resolve its pain by seeking the remedy that brings it back to completion and contentment; or can dissociate from the pain (through, for instance, certain types of defence mechanisms) and descend back into Nafs Ammāra.
Definition of Mental Health
In the author’s perception, Western Psychology generally gives little consideration to defining mental health (Jung is an exception, and in his way, Freud). Islamic Psychology does have a fairly clear conception. Mental Health can be defined, in terms of the model, as that state in which the Self is under the full control of the Qalb which is open to divine inspiration. In effect, this is the same as the Self being in full alignment with the Fiṭra, and being, at least able to access the state of Nafs Muṭmaʾinna.
Al-Ghazali (14) gives the analogy of the rider on a horse. In this analogy, the horse is the Hawā, healthy and operating in its fiṭra; guided by ʿAql (the reins), under the control of the rider who is centred in the Qalb under divine guidance. From this analogy, psycho-pathology can be seen in different manifestations. For example, the horse out of control; the horse under control but by the reins directing it in an irrational way;the horse firmly under control and being firmly guided by the reins to where the rider wants to go but being contrary to fiṭra and destructive.
Diagnosis
The suggested model of the Self (Fig. 1) and understanding of the dynamics operating within the Self (Fig. 2), and the Islamic definition of mental health are all guides to diagnosing pathology. Though a dysfunctionality in one level of the Self is likely to radiate through the other levels, the therapist should have an eye to where the epi-centre of pathology lies, bearing in mind the pathology of the Qalb and the disconnectedness of the body; as well as the interplay between ʿAql and Hawā, which is the almost exclusive focus of mainstream Western Psychology.
Of particular importance, is recognising the difference between low mood associated with a state of remorse (nafslawwāma), – (which is a healthy stage of transition to self-completion and well-being), from low mood as a symptom of pathological depression.
There are two further Islamically distinctive considerations in diagnosis. One, is clarifying whether a person’s problems are resulting from being dissociated from fiṭra, – essentially a pathology of the Qalb; or, whether the problem results from the person being in touch with their fiṭra but living in a society which is not.
The second, is to consider the ‘primary’ as well as the ‘secondary’ causation of a condition. The primary causation is always God in Islamic thinking, and accepting this leads to a consideration of the meaning of the condition, since nothing is ordained without meaning. The secondary causation refers to the agents that are used to directly cause the condition (e.g. trauma, or inappropriate diet). Al-Ghazali criticised Ibn-Sina for not paying sufficient attention to the primary causation of a disease.
In his Alchemy of Happiness (15), Al-Ghazali gives a good example of the incompleteness in diagnosis that comes from only considering secondary causation. Al-Ghazali describes a man who goes to a physician complaining of feeling low in mood and having lost pleasure in life. The physician diagnoses melancholia and prescribes a medicine. But, says Al-Ghazali, it did not occur to the Doctor that God had so created that state of depression in His servant so that he would return to Him. In other words, the depression (whatever its secondary causes) because it leads to a diminishing of interest in the outer world, facilitates a reconnection with inward spirituality.
Therapy
The goal in Islamic therapy is to bring the client back to a state in which they are connected to their Qalb (heart), in which state the client can access their own internal guidance. Or, at least, the therapist should aim to remove obstacles to achieving that state, and avoiding putting obstacles in the way. This understanding relates to the goals of Jungian Psychotherapy.
The author knows of three studies (16,17) which researched what factors Muslim Psychotherapists regarded as the most important variables in healing. All three studies found that it was the inner state of the therapist that was regarded as the most important factor. If the therapist is in touch with their heart, this seems to facilitate the client reaching the same state.
Beyond this, any therapy from whichever tradition, that does not conflict with the Islamic paradigm can be used. As the hadith states, “all knowledge is the property of the Believer”. However, caution needs to be exercised with any therapy that derives from Freud. As Badri articulated in his 1979 publication (6) Freud’s psycho-analytic theory can be toxic for Muslims, (which is not to say some of Freud’s clinical observations do not have validity). Caution also needs to be exercised with the mindfulness techniques derived from Buddhism to avoid a state in which mind controls mind to the point that a dissociation is produced, both from the Qalb and from outer life. There are, however, Islamically sound practices of ‘contemplation’ which are entirely sound (4) and which open up the heart.
It is worth noting that caution needs to be exercised with techniques, such as N.L.P., which strongly strengthens the ‘will’ as the effect of such techniques can make it more difficult to be in a state of submission to the Qalb. In moderate doses with some conditions, such techniques can be useful; – but with regard to what Ibn Sina said, – that a skilled physician can use a poison if all else fails providing he is careful with the dose.
As Islamic Psychology pays attention to the inner spiritual part of the Self, and to the subtle relationship of the body with spiritual and mental states, a holistic Islamic Psychological therapyshould also be able to access various therapies that includes Quran recitation, Ṭibb, Ḥijāma (cupping), the sunnasports; and traditionally, music, scent, colour and architecture. In the West, these are not normally regarded as part of the psycho-therapeutic repertoire.
References
- Badri M. Cultural and Islamic Adaptation of Psychology: A Book of Collected Papers. Human Behaviour Academy; 2017.
- Enriquez VG, Philippine Psychology Research and Training House. Indigenous psychology : a book of readings. Diliman, Quezon City, Philippines: Philippine Psychology Research and Training House; 1990.
- Skinner R, Kaplick PM. Cultural shift in mental illness: a comparison of stress responses in World War I and the Vietnam War. JRSM Open. 2017;8(12).
- Badri M. Contemplation: An Islamic Psychospiritual Study. International Institute of Islamic Thought (IIIT); 2000.
- Badri M. Abu Zayd al-Balkhi’s Sustenance of the Soul: The Cognitive Behavior Therapy of a Ninth Century Physician. International Institute of Islamic Thought (IIIT); 2013.
- Badri M. The Dilemma of Muslim Psychologists. Islamic Book Trust; 1979.
- Rothman A, Coyle A. Toward a Framework for Islamic Psychology and Psychotherapy: An Islamic Model of the Soul. J Relig Health. 2018;57(5):1731–44.
- Skinner R. Traditions, Paradigms and Basic Concepts in Islamic Psychology. Skinner R, editor. J Relig Health. 2018;58(4).
- Kaplick PM, Skinner R. The Evolving Islam and Psychology Movement. Eur Psychol. 2017;22(3):198–204.
- Rothman A. An Islamic Theoretical Orientation to Psychotherapy. In Templeton Press; 2018.
- Gianotti TJ. Al-Ghazali’s unspeakable doctrine of the Soul; unveiling the esoteric psychology and eschatology of the Ihya. Brill; 2001.
- Jung CG. The red book. New York, NY, US: W W Norton & Co; 2009.
- Mahmoud S. The Paradigmatic Nature of the Ritual Prayer in Ibn Arabi. [Doctoral Thesis]. University of Cambridge; 2012.
- Al-Ghazali AH. The book of knowledge. Adam Publishers; 2009.
- Ghazzali AH. The Alchemy of Happiness. Chicago, IL: Great books of the Islamic World.; 2008. 1003 p.
- Pasha H. Ideological and social representations of mental health and counselling [M.Sc]. [L.S.E London University]; 2003.
- Maynard S. Muslim Mental Health [Internet]. 2006. Available from: http//de.scribe.com/doc/90034306/Muslim-mental-Health-Stephen-Maynard
