
Abstract
A simple look at the demographics of our world today bears testimony to the influence that Islam has had on our planet and with close to 2 billion adherents, it is safe to conclude it is a vast one. However, Islam’s influence in our world is not merely limited to population size but extends and encompasses a huge scope of disciplines and sciences. Islam aims to develop humanity in every arena of life through the guidance given in the Qur’an and Hadith. These both served as the basis for the Islamic Golden Age between the 10th and 18th centuries. The influence on medicine was vast, including anatomical dissection, the focus of this article. Many books authored by Muslims were being translated and taught all over Europe; Al-Zahrawi’s book Al-Tasrif served as a key reference for medical knowledge in Europe for many centuries. The Islamic Golden Age ushered in huge changes to clinical practice due to the development of new technologies, instruments, and techniques by Islamic Golden Age physicians as well as the incorporation of the Islamic spirit within the practice of medicine by said physicians. This article will examine the progression of anatomical knowledge and how the knowledge developed or transmitted from the Islamic Golden Age has major implications for modern day practice.
Introduction
Anatomical research and dissection studies have been widely encouraged throughout Islamic History as another discipline to increase in knowledge and master. Muslim scholars in the East as part of the Baghdadi Caliphate translated and built upon the Roman and Greek works (1) with scholars such as Al-Razi, Al-Majusi, and Ibn Sina significantly contributing to the development of medicine and surgery in this era (2). Meanwhile, Muslim physicians and philosophers including Al-Zahrawi, Ibn Zuhr and Ibn Rushd were the most influential physicians in the western regions particularly the Cordoban Caliphate (3). Books such as Al-Zahrawi’s Al-Tasrif were significant as they introduced innovations in the transmission of medical knowledge (4). Al-Tasrif discussed modifications to dissection techniques with detailed diagrams detailing case histories and spanning many chapters in a systemic regarding different ailments and their respective surgical and medical treatments.
Some people have tried to diminish these remarkable feats by claiming that Arabs and Muslims Scholars were only translators of other cultures and did not contribute any new developments to medicine. It is certainly a travesty of justice to support such a ridiculous notion when there are such clear examples to the contrary, among them being the 11th-century Iraqi scientist Ibn al-Haytham, who developed a radically new concept of human vision which differed from old Greek theory. Ibn al-Haytham’s detailed description of ocular anatomy forms the basis for his theory of image formation derived from this fundamentally new theory from experimental investigations (5)(6). His Book of Optics was translated into Latin in the 12th century and continued to be studied both in the Islamic world and in Europe until the 17th century. Ibn al-Nafis, a 13th-century Syrian physician, re-addressed the question of blood movement in the human body referring to evidence derived from anatomical dissection, Ibn al-Nafis described and concluded, that the blood in the right ventricle must be carried to the left by way of the lungs and not through invisible passages in the septum as Galen said (5)(7). The present paper aims to review the history of anatomical dissection with respect to the Islamic Golden Age specifically.
The disciplines of medicine, surgery and anatomy provided an exemplar display of God’s intricately beautiful and detailed creation to its students. Ibn Rushd mentions in his book Fasl Al Maqal, “Knowledge of the ways of creation leads to intimate knowledge of the Creator. The better you know these ways the more intimate your knowledge of the Creator will be.” He observed that a person who studies anatomy must increase his belief in God. Many of his colleagues would have also considered the study of anatomy not only as indispensable to their professional advancement, but also to understand the wisdom and perfection of God’s design of the human being (5). However, the relationship between Islam and human anatomical dissection is a bit more complex as they can be performed on either a living or a dead body. The issue mainly lies regarding the use of anatomical dissection in human cadavers as opposed to surgical dissection. Therefore, before continuing to discuss the contribution of the Islamic Golden Age to the development of dissection, it is important to contextualise and address Islamic beliefs regarding dissection of the human body.
Autopsy:
Autopsy refers to the dissection of a dead body, specifically a human cadaver. Today, it is done for two main reasons which are medical education in hospitals and legally in forensic investigations to determine the cause of death. Some scholars argue that human anatomical dissections cannot be justified within the Islamic framework as the body must be purified and undergo the burial process swiftly. However, the Qur’an and Hadith do not directly address the issue of autopsy which has led to differing interpretations regarding its use. This is demonstrated even within the thinking of the Golden Age physicians, human dissection was not practiced in early Islam, but was in later periods. Some Muslim physicians dissected bodies for education and learning, such as Salahuddin’s physician Ibn Jumay, Abd Al-Latif, Ibn Zuhr and Ibn Rushd with the latter stating that: “Anyone who practices anatomy will increase his faith in Allah” (8). By contrast, Ibn al-Nafis stated that “precepts of Islamic law have discouraged us from the practice of dissection, along with whatever compassion is in our temperament” (9). When the Nile River dried up and there was much starvation, Mowafak al Bagdadi had numerous dead bodies on which to practise his anatomical dissections. It was these very dissections that enabled him to discover and prove that the mandible consists of one part, not two, as Galen had previously postulated. He noted, “I am sure now it is one bone part – mandible… after I had dissected about 2000 human skulls, and it is opposite of what Galen said” (10).
Attitudes towards autopsy have changed over time with the viewpoint of permissibility gaining greater prominence in recent years. Prior to the 10th century, dissection was not performed on human cadavers (11). Autopsy dissection had then been approved by the highest Islamic commissions. Yet out of respect for the dead and the feelings of the deceased’s families, many scholars chose not to carry out these dissections, instead preferring animal dissections. Some did dissect human cadavers, but in secret settings, while others did it with government support. In 1952, the head of Al-Azhar in Egypt stated regarding autopsy that “Necessity permits the forbidden,” thus allowing autopsies in cases of criminal investigations (12).
Surgical Dissection:
Having now covered autopsy dissections and the Islamic viewpoint through history regarding this briefly, now this article will look at surgical dissections on live patients. The golden rules in use more than 1000 years ago are still the same basics for learning and developing medical and surgical skills in our time. For example, improving our neurosurgical skills now depends on one approach: practising in the lab, studying anatomy, and cadaver dissection. This practice gives us the right experience to carry out our work, and it is the same principle used ten centuries ago by Islamic and Arabic scholars in medicine. In the introduction to his book, al-Zahrawi pointed out that good practice in surgery requires a sound knowledge of anatomy or the patient’s life will be in danger (13). To give this remarkable civilisation its due right, a more thorough analysis needs to be undertaken, looking in detail at what the most famous of its contemporaries have achieved in the field of anatomical dissections.
Al-Razi (Rhazes 850-923):
Firstly, we will cover Abu Bakr Al-Razi (Rhazes 850-923). Al-Razi’s contribution to neuroanatomy is well documented in his works which most notably include Kitab al-Hawi fi al-Tibb and Kitab al-Mansuri fi al-Tibb. He described nerves as having both motor and sensory functions and as originating in pairs from the brain and spinal cord with membrane coverings (14). He was the first physician to describe the phenomenon of concussion (14, 15) and in his books he dedicated section to teaching his students to avoid injuring the small nerves drooping eyelid during making the surgical flap stating: “The surgeon must therefore know the anatomy of the nerves, the veins, and the arteries, so as not to sever them by mistake (16, 17). Al-Razi also stated that there were seven cranial and thirty-one peripheral nerves, assigning them the order initially given by Galen. He divided the peripheral nerves into eight cervical pairs, twelve thoracic pairs, five pairs in the lumbar spine, and three in the sacral spine, and he used this knowledge of segmental nerve innervations to localise lesions in patients. (18). He had a patient who complained of numbness of his little finger after neck trauma. He said this patient must have a problem in the last cervical vertebra because he knew from his anatomical studies that the nerve from the last cervical vertebra goes to that finger. Al-Razi described the ascending laryngeal nerve and noted there might be two or double branches on the right side.
Al-Majusi (Haly Abbas 930–994):
Next was Al-Majusi (Haly Abbas 930–994) who was a Persian physician and psychologist whose Kitab al-Malaki (The Royal Book) has been credited with outperforming Al-Razi’s Comprehensive Book of Medicine and Ibn Sina’s Canon of Medicine in some respects. It was one of the earliest illustrations of surgical approaches to skull fractures and other disorders. In addition to discussing internal diseases, he also discussed their treatments and causes. Between the 10th and 13th centuries, the medical school at Salerno, Europe’s centre for medical training, used Kitab Al-Malaki as a core text. While he was in Baghdad’s Buwayhid dynasty, al-Majusi had the responsibility of royal physician. Throughout his writing, he frequently refers to Allah, indicating a deeply religious person (19).
Figure 1: The anatomical sections of the Canon of Medicine by Ibn Sina
Figure 2: Excerpt from Al-Majusi’s Royal Book
Al-Zahrawi (Albucasis 930–1013):
Al-Majusi’s contemporary was none other than Al-Zahrawi (Albucasis 930–1013). Born in Cordoba, Spain, he was an Islamic physician who was considered by many to be the “father of modern surgery”. Al-Zahrawi is most well-known for his revolutionary book Al-Tasrif which was finalised in 1000 AD and covers a wide variety of medical related fields (20, 21). Among the oldest books containing diagrams of surgical instruments, Al-Tasrif was also an illustrated encyclopaedia of medicine and surgery which described operations and interventions for varicose veins, skull fractures, teeth removal, and forceps deliveries. As one of the most systematic and practical medical treatises of the era, Al-Tasrif noted a few differences between that which Al-Zahrawi saw regarding anatomy and from what Galen and other predecessors had seen. In the introduction to his book, Al- Zahrawi pointed out that good practice in surgery requires a sound knowledge of anatomy (22). He greatly contributed to the advancement of medicine and surgery throughout Europe, both in the East and the West with his concepts continuing to influence the practice of surgery even now (23). During the 12th to 17th centuries, Al-Tasrif was used as the textbook for medical education in most European universities instead of Ibn Sina’s The Canon of Medicine. Al-Tasrif made mention of creating incisions, healing of wounds through cauterisation, burning wound with a red-hot steel rod to decrease bleeding and reduce the probability of infection, and bone-setting (22). To further prevent post-surgical infection, he recommended that the wound be regularly cleaned with wine, oil of roses, salt water, or vinegar (24). These books comprise a range of components of surgical therapy in detail based totally on Al-Zahrawi’s personal experiences of the surgical operations alongside more than 200 illustrations of instruments’ designs. Al-Tasrif also includes a section regarding treatment of gynecomastia which serves as the perfect example of how Islamic Golden Age knowledge was innovative and has had far reaching effects even today in modern surgery.

Figure 3: Al-Zahrawi blistering a patient in the hospital at Córdoba
Gynecomastia refers to the phenomenon of breast enlargement in males via many different aetiological causes. Although this condition was recognised since Ancient Greece, no historical evidence exists of any surgical treatment for gynecomastia before Paulus of Aegina. Later in the Islamic Golden Age, Al-Majusi described surgical management of gynecomastia in his Kitab al-Maliki (The Royal Book) and Al-Zahrawi spoke at length regarding gynecomastia treatment in his book Al-Tasrif. The accusation was levelled at that their works were mostly copies of Paulus of Aegina (25). However, the technical innovations and differing modifications of the surgery and associated medicinal remedies found in Al-Tasrif give more credence to the idea that Al-Zahrawi’s accounts were based on his own experiences in surgery. Al-Zahrawi’s surgical methods have remained unchanged for centuries with many sections of his recommendations still indicated in practice today.
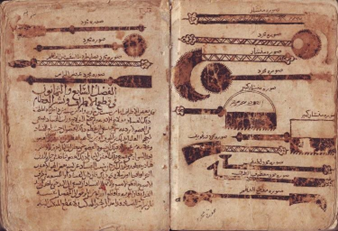 Figure 4: A page of Al-Tasrif depicting the surgical tools devised or utilised by Al-Zahrawi
Figure 4: A page of Al-Tasrif depicting the surgical tools devised or utilised by Al-Zahrawi
According to Al-Zahrawi, there are two innovative surgical techniques to correct gynecomastia. Unlike Paulus of Aegina’s previous recommendation of incision below the breast (26), Al-Zahrawi’s first method would possibly provide breast uplift in addition to lunate incisions over the breast. The second surgical approach described by Al-Zahrawi for the surgery of gynecomastia involved making two lunate incisions along the upper segment of the breast to allow the removal of subcutaneous fat (26). Uniquely, Al-Zahrawi advocated and practised adding powder made from natural substances over the surgical wound to accelerate healing, he mainly used styptic powder, but other substances used included aloe vera, sarcocolla and gum Arabic tree (27). Interestingly, these substances have been shown much later to be effective antimicrobial agents and promote wound healing. It’s worth noting that Al-Zahrawi clearly identified bleeding because of gynecomastia surgery, and as a result, he recommended compression cotton dressing (28). These examples are a remarkable demonstration of Al-Zahrawi’s advanced pharmacological knowledge and surgical prowess which was far ahead of his time (29).
Ibn Zuhr (Avenzoar 1091-1162):
Ibn Zuhr (Avenzoar 1091-1162) was a physician from Andalusia most well-known for his book Kitab Al-Taysir which covered many aspects of treatment including medicine and surgery as well as improving diet for certain conditions. His most significant contribution in this discipline is his use of experimental trial-and-error approach in evaluating novel or controversial surgical procedures for the first time. For centuries, the role of tracheotomy in the resuscitation of life-threatening asphyxia owing to upper airway obstruction was debatable. It was only until the Islamic era, when AI-Razi and later Ibn Sina began to speak positively regarding the benefits of tracheotomy in certain cases and helped to further develop the technique (30)(31)(32).Despite the fact that AI-Razi described tracheotomy as a last resort, he reported witnessing patients with wounds in their throats through which breath was expelled; yet, the patients lived and made a full recovery. However, the dispute relating to its use raged on and thus Ibn Zuhr decided to conduct a tracheotomy on a live goat to settle the debate and demonstrate that tracheotomy is a safe procedure (33). He felt that tracheotomies were not being performed on patients who desperately needed them because of the controversy surrounding its use (34). Ibn Zuhr’s use of an experimental animal model to solve a clinical problem was a predecessor to the strategy used to establish many modern surgical methods. Following him in the 13th century, writers such as AI-Baghdadi (35) and Ibn Al-Quff (36) advised tracheotomy without reservation in life-threatening upper airway blockage that could not be eased by other methods, detailing the procedure in more depth.
Other passages of Al-Taysir demonstrate Ibn Zuhr’s inquisitive mentality and his dependence on trial and error to come to conclusions. Faced with the challenge of no effective therapy for individuals with serious lung ulcers, he learned from shepherds that sheep suffer from a similar ailment for which there is a cure. Therefore, he then began performing post-mortem dissections on sheep to investigate ulcerating diseases of the lung (37). Another valuable concept that Ibn Zuhr developed was that of dedicating lots of commitment to educating and training upcoming surgeons to provide them with the necessary knowledge, skills, and experience before they can operate unsupervised. In Al-Taysir, he emphasises the significance of familiarity with the vasculature and organs of the head and neck while dealing with inflammatory swellings of the neck that are ripe and ready to rupture or drain (38). He continues to argue that only those with experience of dissection and sound anatomical knowledge are qualified to perform an operational intervention (39). He not only promoted learning knowledge but also practised implementing it and applying it to solve new problems. In many other places in his book Al-Taysir, Ibn Zuhr displays his level of innovation with instruments and management lines as he modified ophthalmic surgical instruments (40) and invented tubes for orogastric and rectal feeding for oesophageal paralysis patients, rejecting the notion that feeding could ever work by immersion in tubs of soup and milk (41). Furthermore, Ibn Zuhr highlighted his preference for medical management over surgery which marked a significant paradigm shift in surgery where previously there was an eagerness to undertake surgical dissections despite the risks of infection and haemorrhage. An excellent demonstration of this in practice was his reservation towards surgically treating bladder stones, instead favouring medical therapy. He explained in detail the required methods to aid the stone’s natural course or cause its disintegration (42). Thus, he was a great advocate for prophylactic therapies such as medication and even preventative measures looking to improve the diet as options to be explored before considering surgery.
Figure 5: Title page of the Arabic edition of Al-Taysir
Ibn Al-Nafis (1213–1288):
Ibn Al-Nafis (1213–1288) was one of the last great Muslim physicians of this period and hailed from Syria. According to Ibn Al-Nafis, blood flows directly from the heart to the lungs, where it is “purified”- what he was referring to be the oxygenation of the blood in the lungs. This idea contradicts Galen’s belief that blood is shunted from the right to the left side of the heart through septal pores (43). His observations were also based on detailed dissection, but not of the human body as he was among those who took a more sceptical approach to post-mortem dissection. By contrast the first Europeans to describe the pulmonary circulation accurately were Michael Servetus and Realdo Colombo more than three centuries later. Western medicine could have greatly benefited from his hypotheses regarding the cardiovascular system but unfortunately these were not widely circulated. Ibn Al-Nafis’ accomplishments were not brought to the attention of others until William Harvey’s discoveries in 1628 and it was not until van Leeuwenhoek used a microscope in 1676 to study lung parenchyma that Ibn Al-Nafis’ observations were firmly established, with the crucial bit of evidence being the confirmed presence of pulmonary capillaries (44).
Figure 6: Ibn Al-Nafis’ diagrams demonstrating pulmonary circulation
Conclusion:
In the same way as the heritage of the ancients was studied with great respect, non-Muslim scientists, Jews, and Christians in particular, played significant roles within the Islamic Golden Age’s scientific community. It was the open, non-dogmatic atmosphere that encouraged people to engage in debate, share ideas and seek new knowledge by asking questions and examining available evidence (5). In fact, medicine was mainly practiced by Jewish and Christian physicians very early on in Islamic History, a fact that Imam Al-Shafi’i remarked on: “I do not know of any type of knowledge, after the knowledge of what is lawful and what is unlawful, more noble for a Muslim [to acquire] than that of medicine but, alas! They have neglected it—they have neglected one-third of human knowledge—and abandoned it to Jews and Christians” (45). One such example was Uhanna ibn Masaweh (d. 875), known as Joannes Damascenus, the famous Arab scholar who worked with anatomy, and when it was difficult for him to obtain cadavers, he dissected a special type of monkey whose anatomy was very similar to that of the human body. He carried out this dissection in a special room on the river side of Dejlla in Baghdad, and al Khaleefa Al Motasem ordered the monkeys from the Nile valley (present-day Sudan) for anatomical dissections These scholars also included Ishac al Israilie, Honein ibn Ishak (Joannitius 809-873), and many others.
If the Golden Age scholars had only preserved the ancient cultures without adding anything to them, that would have still marked a praiseworthy contribution to civilization as a whole and the European renaissance. As previously stated, the Arabic versions of the works of Hippocrates and Galen are the only copies that have survived which does demonstrate that the scholars of the Islamic Golden Age did work hard to translate the works of those who came before. But the great efforts of these scholars to develop their own original pieces of knowledge in the fields of anatomy, dissection and surgery cannot be ignored and deserves to be fully recognised in Western academic circles for how vital it has been to the development of modern surgery.
References:
- Ardalan MR, Shoja MM, Tubbs RS, Eknoyan G. Diseases of the kidney in medieval Persia—the Hidayat of Al-Akawayni. Nephrology Dialysis Transplantation. 2007;22(12):3413–3421.
- Golzari SE, Khodadoust K, Alakbarli F, et al. Sleep paralysis in medieval Persia—the Hidayat of Akhawayni (?-983 AD) Journal of Neuropsychiatric Disease and Treatment. 2012; 8:229–234.
- Golzari SE, Mirinejad MM, Kazemi A, Khalili M, Ghabili Avenzoar K. (1092-1162 AD) and Averroes (1126-1198 AD): andalusian Muslim physicians. World Journal of Surgery. In press.
- Al-Ghazal SK. Al-Zahrawi (Albucasis) the Great Andalusian Surgeon. Manchester, UK: Foundation for Science Technology and Civilisation; 2007
- Ingrid Hehmeyer, Aliya Khan, Islam’s forgotten contributions to medical science CMAJ, May 8, 2007, 176(10) |1467
- Russell GA. The emergence of physiological optics. In: Rashed R, editor. Encyclopaedia of the history of Arabic science. Vol. 2. London and New York: Routledge; 1996. p. 672-715. [p. 676, 686-99]
- Ullmann M. Islamic medicine. (Islamic Surveys II). Edinburgh: University Press; 1997. p. 68f.
- Ibn abi Usaybi’a. ‘Uyun al-Anba’ fi Tabaqat aI-Atiba’. Nizar Reda, ed. Beirut: Dar Maktabat al-Hayat, 1965, 530-533.
- Castiglioni A. A History of Medicine. Translated from the Italian and edited by Krumbhaar EB. New York: Jason Aronson, 1975, 258-276.
- Islamic Medical Manuscripts at the National Library of Medicine nlm.nih.gov/
- Mohammed, Madadin; Kharoshah, Magdy (2014). “Autopsy in Islam and current practice in Arab Muslim countries”. Journal of Forensic and Legal Medicine. 23: 80–3.
- J. Davis, B.R. Peterson “Dilemmas and solutions for the pathologist and clinician encountering religious views of the autopsy” South Med J, 89 (11) (1996 Nov), pp. 1041-1044
- Aciduman A, Belen D, Simsek S: Management of spinal disorders and trauma in Avicenna’s Canon of Medicine. Neurosurgery 59:397–403, 2006
- Scott Y Rahimi, Dennis E. Mcdonnell, Amir Ahmadian, John R, Vender. Medieval neurosurgery: contributions from the Middle East, Spain, and Persia
- McCrory PR, Berkovic SF: Concussion: the history of clinical and pathophysiological concepts and misconception. Neurology 57:2283–2289, 2001
- Aziz, E Nathan B, McKeever J: Anaesthetic and analgesic practices in Avicenna’s Canon of Medicine Am Chin Med 28:147-151; 2000
- Gruner OC: A Treatise on the Canon of Medicine of Avicenna. London: Luzac, 1930
- Flamm ES: Historical observations on the cranial nerves. J Neurosurg 27:285–297, 1967
- Haque, Amber (2004), “Psychology from Islamic Perspective: Contributions of Early Muslim Scholars and Challenges to Contemporary Muslim Psychologists”, Journal of Religion and Health 43 (4): 357–377 [370]
- Nabri IA. El Zahrawi (936-1013 AD), the father of operative surgery. Annals of the Royal College of Surgeons of England. 1983;65(2):132–134.
- Al-Rodhan NRF, Fox JL. Al-Zahrawi and Arabian neurosurgery, 936-1013 AD. Surgical Neurology. 1986;26(1):92–95.
- S. SPINKS and G.L. LEWIS, Albucasis, On Surgery and Instruments, Arabic, edition with English translation and Commentary, The Welcome Institute of the History of Medicine, and the University of California Press, The Near East Department, 1972-1973
- Belen, D., & Aciduman, A. (2006). A pioneer from the Islamic Golden Age: Haly Abbas and spinal traumas in his principal work, The Royal Book. Journal of neurosurgery. Spine, 5(4), 381–383. https://doi.org/10.3171/spi.2006.5.4.381
- Pormann PE, Savage-Smith E. Medieval Islamic Medicine. Edinburgh, UK: Edinburgh University Press; 2007.
- Adams F. The Seven Books of Paulus Aegineta. London, UK: Sydenham Society; 1844–1847. On male breasts resembling the female; pp. 334–335.
- Papadakis M, Manios A, De Bree E, Trompoukis C, Tsiftsis DD. Gynaecomastia and scrotal rhacosis: two aesthetic surgical operations for men in Byzantine times. Journal of Plastic, Reconstructive and Aesthetic Surgery. 2010;63(8): e600–e604.
- Zakkour MY. Kitab Al-Zahrawi Fi- Tibb Li Amal Al-Jarraheen (Or Al-Zahrawi’s Book in Medicine for Surgeons) Damascus, Syria: Syrian State Book; 2009.
- Oates SD. Gynecomastia. In: Singletary SE, Robb GL, Hortobagyi GN, editors. Advanced Therapy of Breast Disease. Ontario, Canada: BC Decker; 2004. pp. 44–49.
- Hamarneh SK, Sonnedecker G. A Pharmaceutical View of Abulcasis Al-Zahrāwī in Moorish Spain. Leiden, The Netherlands: Brill Archive; 1963.
- AI-Mazrooa A A and Abdel-Halim R E. “Anesthesia 1000 Years Ago.” Middle East J Anesthesiol., February 2000; 15(4): 383-92.
- AI-Razi M Z. Kitab al-Hawi fi al-tibb. Hyderabad: Osmania Oriental Publications Bureau, 1961, vol. 3: 225-233.
- Ibn Sina a A. Kitab aI-Qanun fi al-tibb. Beirut: Dar Sadir, reprint of Cairo Boulak edition, 1877; vol. I: 334; vol. 2: 200-205.
- AI-Zahrawi K A. In: Spink MS, Lewis CL, eds and trans, Albucassis on Surgery and Instruments. London: Wellcome Institute of the History of Medicine, 1973, 338-339. [h]
- Ibn Zuhr, Kitab al-Taysir fi al-Mudawat wa- ‘l-Tadbir li-Marwan Ibn Zuhr, Introduction, Al-Khoori M ed. Damascus: Dar al Fikr Press for the Arab Educational Scientific and Cultural Organization, 1983, 149.
- AI-Baghdadi AA. Kitab aI-Mukhtarat fi al-Tibb. Hyderabad: Osmania Oriental Publications Bureau, 1942-1944; vol. 1: 141; vol. 3: 190.
- lbn al-Quff MYA. AI- ‘Umda fi aI-Jiraha. Ist edn. Hyderabad: Osmania Oriental Publications Bureau, 1936, vol. I, 205.
- Ibn Zuhr, Kitab al-Taysir fi al-Mudawat wa- ‘l-Tadbir li-Marwan Ibn Zuhr, Introduction, Al-Khoori M ed. Damascus: Dar al Fikr Press for the Arab Educational Scientific and Cultural Organization, 1983, 129.
- Lerut, Toni, and Ory Wiesel. “History of esophagectomy for cancer of the esophagus and the gastroesophageal junction.” Annals of translational medicine vol. 9,10 (2021): 897. doi:10.21037/atm-21-676
- Ibn Zuhr, Kitab al-Taysir fi al-Mudawat wa- ‘l-Tadbir li-Marwan Ibn Zuhr, edited by M. al-Khoori. Damascus: Dar al Fikr Press for the Arab Educational Scientific and Cultural Organization, 1983, 27.
- Hirschberg J, Blodi F. The history of ophthalmology. Bonn: J. P. Wayenborgh; 1982.
- Azar, Henry A. The Sage of Seville: Ibn Zuhr, His Time, and His Medical Legacy. Cairo: American University in Cairo, 2008. 72-81. Print
- Ibn Zuhr, Kitab al-Taysir fi al-Mudawat wa- ‘l-Tadbir li-Marwan Ibn Zuhr, edited by M. al-Khoori. Damascus: Dar al Fikr Press for the Arab Educational Scientific and Cultural Organization, 1983, 262
- West JB. Ibn al-Nafis, the pulmonary circulation, and the Islamic Golden Age. J Appl Physiol (1985). 2008;105(6):1877-1880. doi:10.1152/japplphysiol.91171.2008
- Akmal, M et al. “Ibn nafis – a forgotten genius in the discovery of pulmonary blood circulation.” Heart views: the official journal of the Gulf Heart Association vol. 11,1 (2010): 26-30.
- Al-Dhahabi MI. Al-Tibb al-Nabawi (prophetic medicine). Cairo, Egypt: Mutafā al-Halabī [cited in Rahman F (1998). Health and Medicine in the Islamic Tradition (pp. 44–45). Chicago, IL: ABC International Group]. 1961.
